Predominance of Th2 Cytokines in AD
Th2 cytokines play a key role in driving the inflammatory cascade associated with AD.1
Non-lesional Skin
- Due to immune dysregulation, non-lesional AD skin is characterized by subclinical inflammation as well as skin-barrier dysfunction1
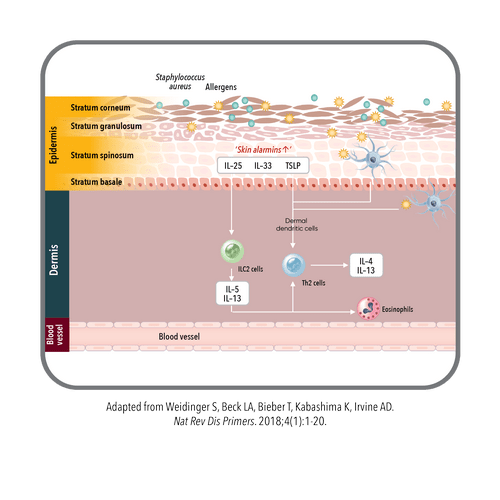
- Dendritic cells take up antigens and amplify type 2 immunity cytokines1
- Worsened skin-barrier dysfunction can stimulate keratinocytes to further promote type 2 inflammation through the release of skin alarmins, such as IL-25, IL-33, and TSLP, which stimulate ILC2s to release more type 2 cytokines such as IL-13 and IL-51

Acute Lesional Skin
- Acute lesional skin is characterized by a reduced expression of important skin-barrier proteins and lipids involved in maintaining skin-barrier integrity1
- The damage caused to the skin barrier triggers the release of further skin alarmins, expanding and activating skin-resident ILC2 cells to produce more cytokines, attracting more immune cells, and amplifying the inflammatory response, including the recruitment of more eosinophils, Th2 cells, and Th22 cells—producing more cytokines1
- Both IL-33 and TSLP, as well as the downstream Th2 cytokines (IL-4, IL-13, and IL-31), act directly on cutaneous sensory neurons, activating itch signaling and leading to scratching1
- During an AD flare there is a decreased microbial diversity, with increased presence of Staphylococcus aureus1

Chronic Lesional Skin
- In the chronic stage, a mixed T-cell infiltrate, including Th1 and Th17 cells, perpetuates skin inflammation and promotes skin remodeling and fibrosis1
- Repetitive scratching leads to lichenified (thickened) skin1
IL-13 plays a key role in AD signs and symptoms, including skin barrier defects and infections, inflammation, skin thickening, and promoting the itch-scratch cycle.2-9
- Weidinger S, Beck LA, Bieber T, Kabashima K, Irvine AD. Atopic dermatitis. Nat Rev Dis Primers. 2018;4(1):1-20.
- Howell MD, Kim BE, Gao P, et al. Cytokine modulation of atopic dermatitis filaggrin skin expression. J Allergy Clin Immunol. 2007;120(1):150-155.
- Kim BE, Leung DY, Boguniewicz M, Howell MD. Loricrin and involucrin expression is down-regulated by Th2 cytokines through STAT-6. Clin Immunol. 2008;126(3):332-337.
- Berdyshev E, Golvea E, Bronova I, et al. Lipid abnormalities in atopic skin are driven by type 2 cytokines. JCI Insight. 2018;3(4):e98006.
- Nomura I, Goleva E, Howell MD, et al. Cytokine milieu of atopic dermatitis, as compared to psoriasis, skin prevents induction of innate immune response genes.
J Immunol. 2003;171(6):3262-3269. - Purwar R, Werfel T, Wittmann M. IL-13-stimulated human keratinocytes preferentially attract CD4+CCR4+ T cells: possible role in atopic dermatitis. J Invest Dermatol. 2006;126(5):1043-1051.
- Oetjen LK, Mack MR, Feng J, et al. Sensory neurons co-opt classical immune signaling pathways to mediate chronic itch. Cell. 2017;171(1):217-228.e13.
- Moriya C, Jinnin M, Yamane K, et al. Expression of matrix metalloproteinase-13 is controlled by IL-13 via PI3K/Akt3 and PKC-δ in normal human dermal fibroblasts.
J Invest Dermatol. 2011;131(3):655-661. - Mack MR, Kim BS. The itch-scratch cycle: a neuroimmune perspective. Trends Immunol. 2018;39(12):980-991.